
Add a video
Caregiver Mini-Course

What’s happening in the brain and why understanding the processes changes your perspective and how you care for your loved one.
You Are Not Alone
Lesson Three
What's actually happening in the brain — and why understanding it changes everything about how you care.
Lesson 2 gave you the physical tools — how to position, how to read pain, how to make the environment safer and more comfortable. This lesson goes somewhere different.
This lesson asks you to step inside the brain of the person you're caring for. Not to diagnose. Not to become a clinician. But to understand — really understand — what they are experiencing when they forget, when they resist, when they seem afraid of things that don't make sense to you.
Because once you understand what's happening neurologically, the behaviors that feel the most confusing and exhausting begin to make complete sense. And when things make sense, caregiving gets a little bit easier to bear.
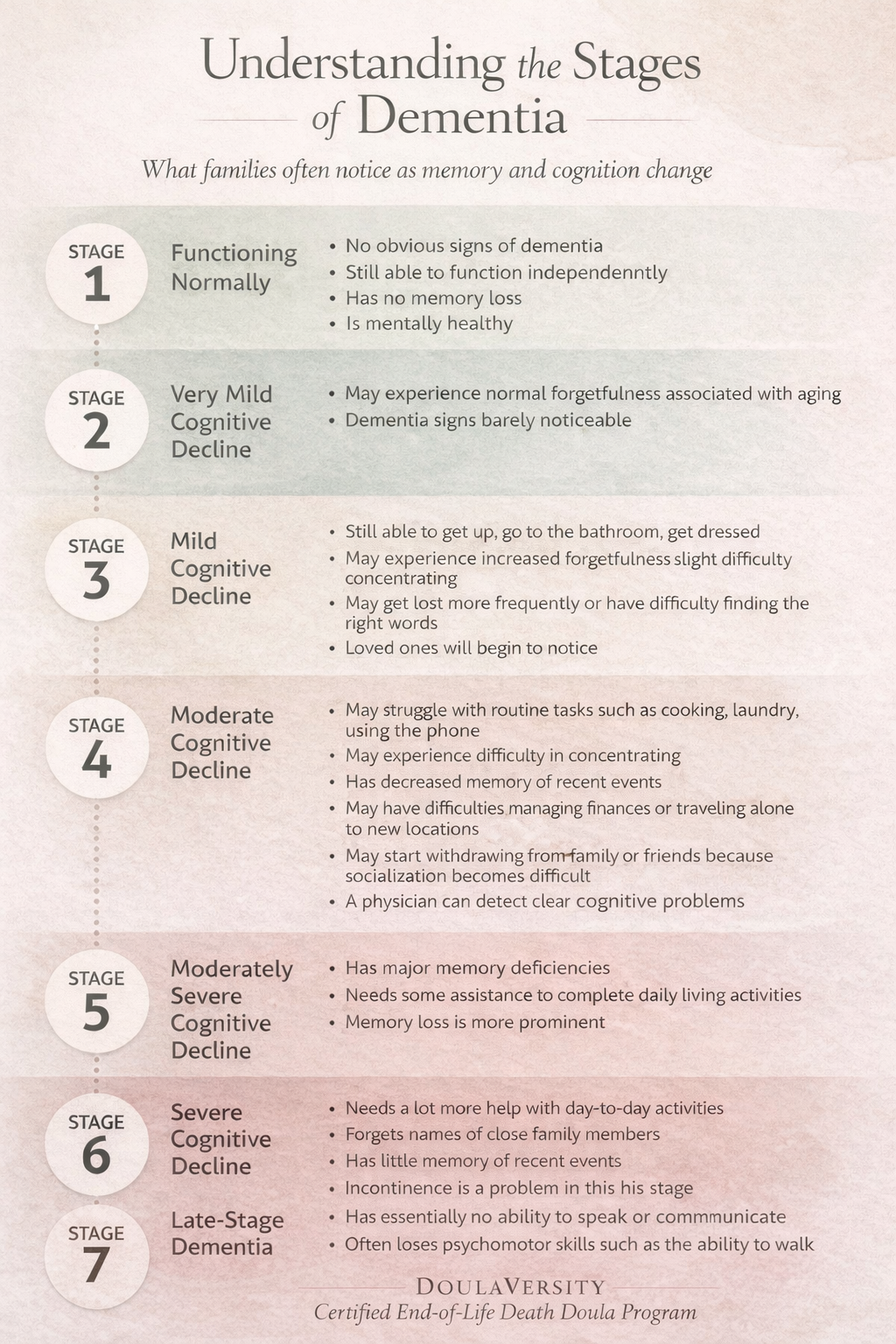
When most people hear the word "dementia," they think of forgetting. Forgetting names, forgetting faces, forgetting where you put your keys. And while memory loss is often part of the picture, it's only one piece of something much larger.
Dementia is brain failure. It is a physical, structural, neurological process happening inside the brain — visible on medical imaging, measurable in cognitive testing, and entirely outside the control of the person experiencing it. It is not about willpower. It is not about attitude. It is not a normal part of aging, and it is not something a person can simply try harder to overcome.
Understanding this distinction matters enormously — not just intellectually, but emotionally. Because when we understand that the behaviors we're seeing are the result of an organ failing to do its job, something shifts in us. The frustration doesn't disappear entirely, but it softens. And that softening is one of the most important things that can happen in the caregiver relationship.
"For a long time I thought she was being stubborn. That if she just tried harder she could remember. My hospice nurse finally explained what was happening in her brain — and I cried, because I realized she was trying. Her brain just couldn't do it anymore."MRI scans allow providers to see real, structural changes in the brain that correspond to dementia. These aren't abstract or invisible — they are physical changes you can see on a scan. This matters because it gives visible evidence of what is a physical illness, not a personality problem.
The Bottom Line
MRI doesn't diagnose dementia alone, but it gives visible, physical evidence of brain failure — reinforcing that dementia is an illness, not a character flaw and not a choice. When you find yourself frustrated by a behavior, return to this: the organ responsible for that behavior is failing. It is doing the best it can.
"Dementia" is not one condition. It is an umbrella term — a category that holds many different types of brain failure, each with its own pattern of progression, its own earliest symptoms, and its own particular challenges for caregivers.
This is why no two people with dementia behave the same. And it's why what works beautifully for one person may not work at all for another.
The most familiar type. Begins with memory, orientation, and communication changes. Progression is gradual and follows a relatively predictable pattern over years.
Caused by reduced blood flow, strokes, or vessel damage. Often progresses in steps — periods of stability followed by sudden decline after a vascular event.
Includes visual hallucinations, significant movement changes similar to Parkinson's, and dramatically fluctuating alertness — sometimes within the same day.
Affects speech, judgment, impulse control, and personality long before memory. Often misdiagnosed as a psychiatric condition in its early stages.
A blend of several types — most commonly Alzheimer's plus vascular. Very common, especially in older adults, and creates overlapping symptom patterns.
Parkinson's-related dementia, chronic alcohol-related dementia, rare genetic forms, and more. The category is wide — and the presentation varies accordingly.
Why This Matters for You
Knowing the type of dementia your loved one has helps you anticipate what's coming, understand current behaviors, and communicate more effectively with their care team. If you're not sure of the diagnosis, it's worth asking. "What type of dementia does she have, and what does that typically look like as it progresses?" is a completely reasonable question to bring to any appointment.
Even for people who never had a formal dementia diagnosis, end-of-life decline can bring dementia-like symptoms — driven by organ failure, decreased oxygenation, reduced nutrition, medication changes, and multisystem decline. The brain is sensitive to all of these, and as the body winds down, cognitive changes are nearly universal.
What follows are the patterns caregivers encounter most often. The goal isn't to give you a checklist to track — it's to help you recognize what you're seeing and understand where it's coming from. Because when behavior has a neurological explanation, it stops feeling personal.
Some days they recall specific details; other days they can't place familiar faces. This variability is neurological, not performance. The brain accesses memories unevenly as pathways break down.
Delayed answers, difficulty following conversations, repeating the same question minutes apart. The processing speed of the brain has changed — give more time, and don't rush to fill the silence.
Sudden fear, tears, anger, or irritability with no apparent trigger. These are driven by neurological changes, not personality — the brain's emotional regulation systems are affected alongside everything else.
Believing someone is in the house, hiding belongings, or watching them. When the brain can't make sense of the world reliably, it fills in gaps with fear. This is not delusion in the psychiatric sense — it is a failing brain doing its best to explain confusing information.
Thinking it's morning at night, wanting to "go home" even when home, mixing past and present. Time orientation is one of the first things to go — and often one of the most disorienting for caregivers to witness.
Childlike behaviors, agitation, impulsivity, or fixation on certain tasks or phrases. The frontal lobe — responsible for impulse control and personality regulation — is affected by most forms of dementia.
Difficulty with walking, swallowing, continence, or coordination as the brain loses control of body systems. These are not separate from the dementia — they are part of it.
Seeing people, animals, or objects that aren't there — especially common in Lewy body dementia and in the final stages of most types. Arguing about whether they're real is rarely helpful.
A Note on Good Days and Bad Days
One of the most confusing — and sometimes hurtful — aspects of dementia is the inconsistency. They remember something one day that they've forgotten for weeks. They seem completely present, and then an hour later they're somewhere else entirely. This is neurological, not manipulative. The brain accesses what it can, when it can. A good day is not proof they've been exaggerating. A bad day is not backsliding. It is the nature of a brain working unevenly.
We've covered what's happening in the brain globally. Now let's look at something more specific — something that plays out in every room of the home, every single day, and that most caregivers never fully understand until someone explains it to them.
As dementia progresses, the brain doesn't just lose memory. It loses something more fundamental: the ability to interpret what it's seeing.
Two regions of the brain — the parietal and occipital lobes — are responsible for processing visual information. Not just seeing, but interpreting: recognizing edges, judging depth and distance, detecting contrast between objects, and understanding where one surface ends and another begins.
In a healthy brain, this happens automatically and instantly. You glance at a room and immediately know where the floor is, where the furniture is, what's safe to step on, and how far away things are.
In a brain affected by dementia, these systems become unreliable. The eyes may still work perfectly. But the brain can no longer consistently make sense of what the eyes are sending it.
The result is an environment that looks wrong — not dramatically, not like a hallucination, but subtly, in ways that feel deeply unsettling and unsafe to the person experiencing it.
This Is Not Confusion. This Is Not Stubbornness.
This is the brain doing its best with systems that are no longer reliable. The fear is real. The resistance is real. The source of it is neurological — and once you know that, you can stop trying to convince them and start changing the environment instead.
Environmental misinterpretation doesn't just happen at dusk or during a sundowning episode. It can happen anywhere, at any time — and certain rooms and features are especially likely to trigger it. You may notice your loved one:
The Reframe That Changes Everything
When your loved one resists, freezes, or seems afraid — stop asking:
"What's wrong with them today?"
And start asking:
"What is the environment showing their brain that feels unsafe?"
That shift — from person-as-problem to environment-as-problem — is one of the most powerful tools you have. Because the person can't change their brain. But you can change the environment.
Of all the rooms in the home, the bathroom is where environmental misinterpretation most often becomes a crisis. A person who managed their own bathing and toileting for decades may suddenly resist going in. They pause at the doorway. They seem anxious once inside. They refuse to shower. They won't sit on the toilet.
Understanding why — really understanding it, from the inside out — moves you from frustration to compassion. From a power struggle to a partnership.
Bathrooms combine almost every feature that makes environmental interpretation difficult for a declining brain — all in one small space.
Most bathrooms are designed in white. White toilet, white seat, white bowl, white tile floor. For a brain that can no longer detect contrast reliably, the toilet seat blends into the bowl, the bowl blends into the floor, and the entire fixture becomes visually indistinct. Your loved one may genuinely not be able to see it clearly enough to safely lower themselves onto it. Sitting down into something you can't quite locate with your eyes is frightening — and rightfully so.
Shiny tile and reflective surfaces create visual information that a healthy brain dismisses easily. A declining brain cannot. The reflection on a tile floor may look exactly like standing water. Hesitating at the bathroom doorway isn't stubbornness — it's caution in response to what genuinely looks like an unsafe, slippery surface.
When depth perception breaks down, the brain uses contrast as a substitute cue for depth. Dark areas look lower. A dark bath mat on a light tile floor can look like a hole or a sudden drop. Your loved one may step around it, freeze near it, or refuse to enter the room at all. They are not confused about what a bath mat is — they are responding to what their brain is telling them is a gap in the floor.
Self-recognition — the ability to recognize your own reflection — is a cognitive function, not just a visual one. When your loved one looks in the bathroom mirror and doesn't recognize themselves, what they see is a stranger in the room. Someone watching them undress. The anxiety and agitation that follows is completely understandable — from their perspective, it's real.
When your loved one steps into the shower, their brain must simultaneously process the sound of water, temperature changes on the skin, water pressure, steam, shifting reflections, the sensation of standing on a wet surface, and visual distortion. For a brain already working overtime to interpret the environment, this level of input can quickly become overwhelming. Resistance to showering is often not about hygiene avoidance — it's a self-protective response.
You don't need to renovate. You need to make the bathroom more readable for a brain that's lost some of its ability to interpret visual information. Most of these changes are inexpensive, simple, and take less than an afternoon.
A colored toilet seat on a white toilet is one of the highest-impact, lowest-cost changes you can make — it makes the seat immediately visible and can dramatically reduce hesitation. Colored towels near the toilet or shower give the brain visual anchors. A colored grab bar instead of chrome helps it stand out against white walls.
Use a solid-colored, non-slip bath mat rather than a patterned one — patterns can appear to move to a struggling brain. Choose a color that is clearly distinct from the floor but not so dark it reads as a hole. If your loved one keeps stepping around the mat, try removing it temporarily. Non-slip socks may be safer than a mat creating more confusion than it prevents.
Harsh overhead lighting creates deep shadows that look like depth changes or holes. Soft, even, diffuse lighting is the goal. Side-mounted lights near the mirror reduce facial shadows that make self-recognition harder. A nightlight at floor level helps with nighttime bathroom trips and makes the space feel less threatening in the dark.
If your loved one becomes distressed and seems to be reacting to the mirror, covering it is a simple fix. A fabric panel, frosted window film, or even a towel draped over it can eliminate the confusion entirely. You can frame this practically: "I'm reorganizing a bit" — no lengthy explanation needed. If mirror distress only happens at certain times, try covering it only during those windows.
Warm the bathroom before bringing your loved one in. Use a handheld showerhead so you control where the water goes. A shower chair removes the need to balance on a wet surface. Pre-warm the water to eliminate startling temperature shifts. Keep conversation calm and minimal — talking adds cognitive demand. On high-resistance days, a sponge bath is always better than a distressing full shower. Dignity and cleanliness can both be preserved without water.
How You Approach It Matters as Much as the Environment
Go slowly, and narrate gently: "We're going to walk in together. The floor is dry and safe." Let them hold onto you or a grab bar first — physical grounding can orient a disoriented brain before they step in. Watch what they're looking at; their eyes will often tell you exactly what's confusing them. Offer choices whenever possible. Choice restores a sense of control when so much feels out of control.
One of the most painful parts of dementia caregiving is watching the language between you and your loved one change. The conversations you used to have. The inside jokes. The ease of being understood. As dementia progresses, communication requires a different approach — one that meets the brain where it is now, rather than where it used to be.
The most important shift is this: stop trying to bring them into your reality, and start entering theirs.
"She kept asking for her mother. Her mother had been dead for 40 years. I used to correct her, and she'd get so upset. Then I started just saying 'Tell me about your mom.' She'd light up. We'd have these beautiful conversations. I stopped correcting her and started listening."Correcting someone with dementia doesn't restore the memory — it creates distress and shame without any benefit. When they say something that isn't true, gently redirect toward the feeling behind it rather than the factual error. "You miss her. Tell me about her."
If they believe it's 1965, or that their mother is coming for dinner, meet them there. Ask questions. Show curiosity. You are not lying — you are choosing connection over correction. Their emotional experience is real even when the facts aren't.
Short sentences. One idea at a time. Slow your pace and leave space for processing. Don't repeat a question multiple times if there's no answer — give time, then gently try a different approach.
Beginning a sentence with their name helps orient them to who is speaking and that this conversation is for them. "Margaret, I'm going to help you with your shoes." It's grounding, even when little else is.
Your tone of voice, your facial expression, and your body language communicate far more than your words — and these channels stay accessible much longer than verbal language. A calm face and a slow voice can soothe even when words fail entirely.
You don't have to validate the content to validate the feeling. "I can see you're frightened. I'm right here. You're safe." The emotional truth is always real, even when the facts are not.
Repeated questions are one of the most exhausting aspects of dementia caregiving. "When is dinner?" asked fourteen times in an hour. "Where is Dad?" from someone whose husband has been gone for twenty years. It is important to remember that each time they ask, it is the first time — for them. The previous answer did not register because the brain could not retain it.
Answering with frustration doesn't help them — it only adds shame to their already disorienting experience. Try answering the feeling rather than the question. "Dinner is coming soon — you must be hungry. What sounds good?" Or distraction into something engaging. Or simply a warm, patient answer, given again.
When Hallucinations Are Present
If your loved one is seeing or hearing things that aren't there — especially common in Lewy body dementia and late-stage decline — arguing about whether they're real is almost never helpful and often causes distress. Instead: acknowledge the experience without confirming or denying. "That sounds frightening. I'm here with you." If hallucinations are causing distress or putting them at risk, speak with the hospice nurse or physician about whether medication might help.
Communicating this way — with patience, with curiosity, with the same gentle answer for the fourteenth time — is exhausting work. It requires you to set aside your own need to be understood, your grief for the relationship you used to have, and your frustration at a situation you did not choose.
It is okay to step away when you need to. It is okay to feel grief about what language between you has become. That grief is love — and it deserves space, not suppression.
Lesson 3 asked you to do something hard: to step inside a brain that is failing and try to see the world from inside it. That is not a clinical exercise. That is an act of deep love.
You now understand things that most family caregivers never fully understand — what dementia actually is, why the behaviors you're seeing make complete neurological sense, and how the environment itself can become a source of fear and confusion that you have the power to change.
"You are not managing resistance. You are redesigning the environment for a brain that is working as hard as it can. That is not a small thing. That is an act of love."
In Lesson 4, we turn to the final chapter — understanding the body's natural process of shutting down. What happens physically in the weeks, days, and final hours of life. What you will see. What it means. And how to be present for it without fear.
Take the time you need. Come back when you're ready.
Continue to Lesson 4 ↗
